Let’s Address Tooth Loss and it’s Consequences

Top 10 Dental Questions You Should Ask
August 23, 2017
Frequently Asked Questions About Invisalign
September 19, 2017
There are two basic ways to have a tooth removed: You can go to your nearest dentist for a careful extraction, or you can take a serious blow to the face. Unfortunately, many people end up going with option number two. They catch a stray elbow during a basketball game, fall face-first on the sidewalk, or — in rare cases — get in a fist fight.
What should I do if I lose a permanent tooth?
A knocked-out (or, in dental speak, “avulsed”) tooth is an emergency. If you don’t get help soon, it will be impossible to salvage the tooth, and the socket can become badly infected. By taking quick action, you can save both the tooth and the socket.
Here’s what you need to do:
- Find that tooth!
- Pick it up by the crown, not the fleshy root. If the root looks dirty, give it a quick rinse with a sterile saline solution, milk, or saliva. Don’t scrub it or touch it — you could wind up losing vital tissue.
- As unappealing as it sounds, try to put the tooth back in its socket. Then hold it in place with gauze or a clean washcloth until you get to a dentist.
- If the tooth won’t go back in place, put it in a glass of milk or sterile saline solution. Don’t put it in water. (Water doesn’t preserve the tooth as well, which can make it more difficult to reimplant.) You can also carry the tooth tucked between your gum and cheek until you get to the hospital or dentist’s office.
- Get to a dentist immediately. (And don’t forget to bring the tooth!) If a dentist isn’t available, go to a hospital emergency room.
What if my child knocks out a baby tooth?
Unlike permanent teeth, baby teeth can’t be replaced. If your child knocks out a baby tooth prematurely, don’t waste any time looking for it. Instead, comfort your child and help her rinse her mouth out with cold water. Then call a pediatric dentist right away. The dentist won’t be able to save the tooth, but he can give your child pain relievers to make her feel better, and antibiotics to prevent an infection. Your child may also need a spacer, a device that keeps the other teeth from crowding into the newly formed gap. This gives future permanent teeth room to grow.
If my tooth isn’t knocked out but just loosened, should I still see a dentist?
It’s a good idea. Even if the accident left you with only a loose tooth, a dentist’s attention can help reduce the risk that the tooth will die or fall out later.
How can I keep my teeth where they belong?
Sports injuries are a leading cause of knocked-out teeth. If you or your child play any sport with a risk of falls or blows to the face, helmets, face masks, and mouth guards should be standard equipment. According to the American Academy of Pediatric Dentistry, that list includes football, basketball, baseball, soccer, hockey, skateboarding, gymnastics, and martial arts. If store-bought mouthguards aren’t comfortable, you can get a customized one from your dentist.
The Unseen Effects of Tooth Loss
The most obvious effect of missing teeth is aesthetic. The way you look affects the way you feel, and the psychological and social consequences of tooth loss can also be profound, as we shall see. But it’s not just about unsightly gaps; there’s something less apparent going on in the area of a lost tooth that can affect function, health, facial aesthetics — just about everything.
Believe it or not, in the beginning, and at the end — it’s not so much about teeth as it is about bone, which needs stimulation to maintain its form and density. In the case of alveolar (sac-like) bone which surrounds and supports teeth, the necessary stimulation comes from the teeth themselves. Teeth make hundreds of fleeting contacts with each other throughout the day. These small stresses are transmitted through the periodontal ligament (“peri” – around; “odont” – tooth) that suspends each tooth in its socket, prompting the bone to remodel and rebuild continually.
When a tooth is lost, the lack of stimulation causes loss of alveolar bone — its external width, then height, and ultimately bone volume. There is a 25% decrease in width of bone during the first year after tooth loss and an overall 4 millimeters decrease in height over the next few years.
As bone loses width, it loses height, then width and height again, and gum tissue also gradually decreases. Ability to chew and to speak can be impaired. The more teeth lost, the more function is lost. This leads to some particularly serious aesthetic and functional problems, particularly in completely edentulous (toothless) people.
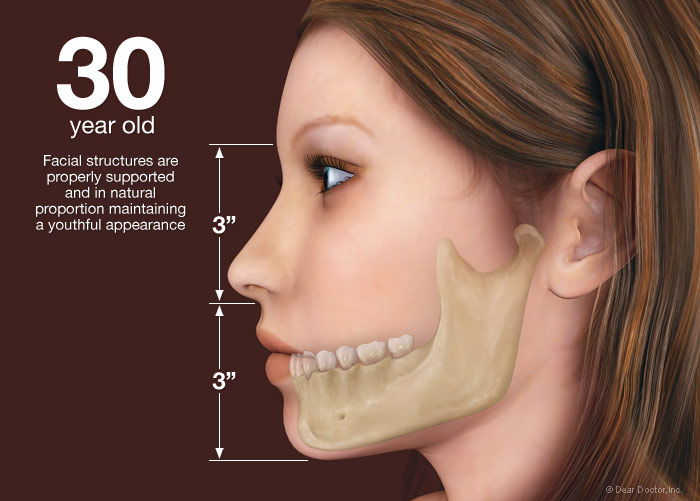
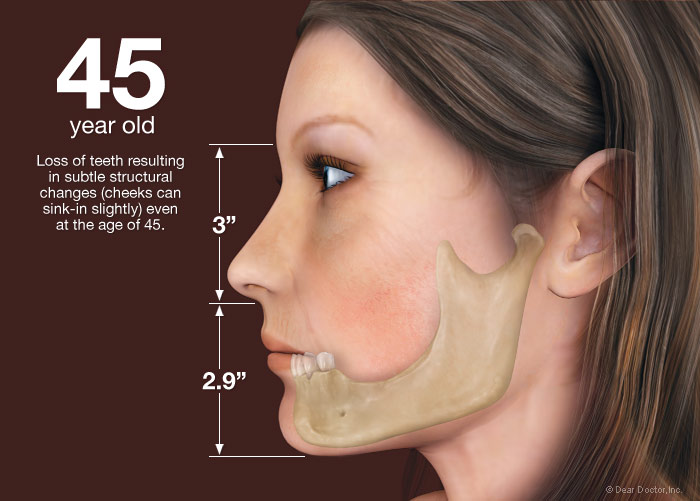
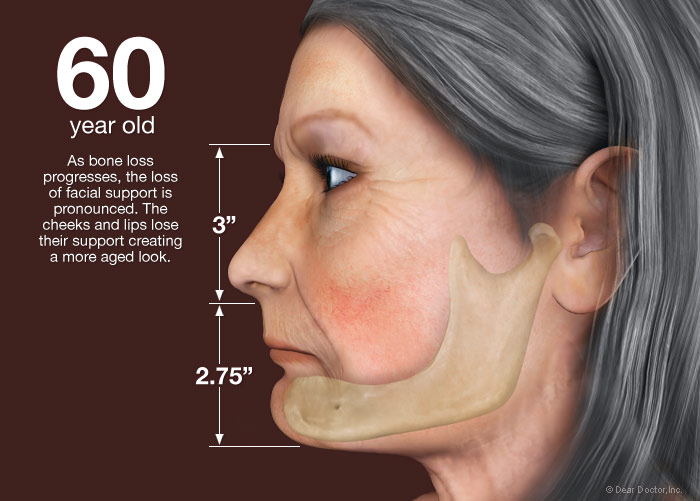
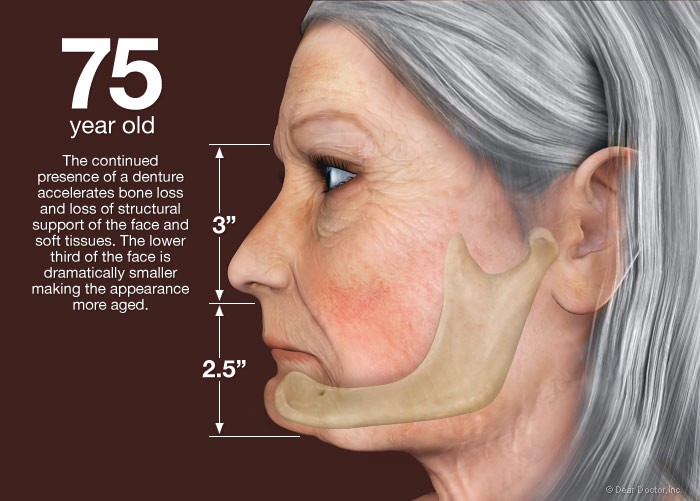
And it doesn’t stop there. After alveolar bone is lost, the bone beneath it, basal bone — the jawbone proper — also begins to resorb (melt away). The distance from nose to chin decreases and with it, the lower third of the face partially collapses. The chin rotates forward and upward, and the cheeks, having lost tooth support, become hollow. Extreme loss of bone can also make an individual more prone to jaw fractures as its volume depletes more and more.
So-called bite collapse can occur when only some of the back teeth, which support the height (vertical dimension) of the face, are missing. This can cause the front teeth to be squashed or pushed forward. They were not designed to support facial height or to chew food — only to hold and incise or tear it. Toothless people appear unhappy when their mouths are at rest because their lips, too, have sagged; unsupported by teeth and gum tissues they just cave in. Without teeth present, the tongue spreads into the space and the face collapses. The same is true of self-confidence.
The First Teeth To Go
In Canada, 70% of the population is missing at least one tooth, usually a back tooth. The first, or “6-year molars” are the first permanent (adult) teeth to erupt into the mouth and, unfortunately, are often the first teeth to be lost — as a result of decay, failed endodontic (root canal) therapy or fracture. In addition, they often have one or more crowns, which are still susceptible to recurrent decay. Longevity reports for crowns vary widely. The mean life span at failure of a crown has been reported as 10.3 years. Other reports range from a 3% failure rate at 23 years to a 20% failure rate at 30 years. Ultimately heavily restored and root canal treated teeth fail to recurrent decay, infection, structural failure or fracture. These teeth are at risk for extraction as a result of these complications, which are the leading causes of single posterior (back) tooth loss in adults.
Up until now, the most common — but not necessarily the best — option for replacing a single back tooth has been a three-unit fixed partial denture (FPD), also called a fixed bridge. In this case, the two teeth on either side of the gap, known as abutment teeth, are crowned and the two crowns together support a “pontic” — a false tooth in the middle (from the French word for bridge). This type of prosthesis (false replacement) can be fabricated within one to two weeks and provides normal shape, function (eating, talking and smiling), comfort, aesthetics and health. Because of these benefits, FPDs have been the treatment of choice for the last six decades. Every dentist is familiar with how and when to use them; they are widely accepted by the profession, the public, and dental insurance companies.
FPDs are not invariably successful over time. If not well maintained, the pontics can act as reservoirs for bacterial biofilm and the abutment teeth can decay. As a result, the supporting abutment teeth are susceptible to structural failure from decay, failed endodontic therapy and/or fracture, increasing their risk of loss.
The abutment teeth of FPDs may be lost at rates as high as 30% within 14 years. Such unfavorable outcomes of FPD failure include the need to replace them and the loss of an abutment tooth or teeth.



{kind=link}
{kind=link}
{kind=link}